Chapter 6
The Aftermath of A TBI
“No one told me it was impossible, so I did it,”
Jean Cocteau
The plausible aftereffect traumatic brain injury has on individuals. I talk about my left side paralysis (e.g., arms and legs) and how some muscle tone is transferred to right side. I also address inability to communicate effectively, my coordination, my continued therapies even till this very day, and other characteristics associated with a traumatic brain injury. It is important to note that I sustained a traumatic brain injury that caused a lot of shearing to my brain. That is why my traumatic brain injury was so tragic to my life.
https://www.youtube.com/watch?v=55u5Ivx31og
After being released from the hospital on May 13, 2004 I did not want to even think about how hard I would have to work to get part of my life back. I was finally home from the Hotel (e.g., St. Vincent) from Hell. Please do not misconstrue that comment about the hospital. The hospital has been amazing in regard to my physical, mental, and social well-being. After two days of seeing my friends and playing with my dog, Kenya, I was going back to Marinette High School just for the last week of classes before I had to start my daily trips (e.g., five times a week) with someone driving back to the hospital in Green Bay.

First I will focus on my physical aspect. After I sustain a brain injury I was left with excess muscle tone. I truly believe that this is where all my problems stem from having excess muscle tone. This is stated because if I did not have hypertone I would be able to strengthen my weak muscles. Before I get into the physical aspect of things I need to explain why after sustaining a traumatic brain injury individuals have excess muscle tone.
Using an evolutionary psychology perspective on muscle tone make a lot of sense when explained this way. It is a bodies natural defense to tighten up and fight or flight when ready for battle or scared. Nearly 200,000 years ago when the first Homo sapiens started to roam the earth he or she had to fight or flight to survive. In order to do such things a person had to flex his or her muscles. Which results in a feeling of muscle tightness or rigidity because who knew what was going to attack a person. When a person, in current times (e.g., the last 100,000 years), would suffered some event to his or her body it would make sense to have mass amount of muscle tightness and that is where muscle tone comes from our ancestors. Our ancestors would see a creature that would eat them if he or she did not flee or fight the predators.
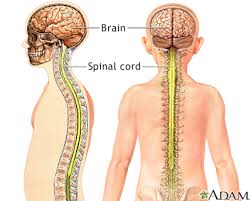
What are the two components that every human needs to survive? If a person would say a brain and spinal cord he or she would be correct. Much of the brain’s job involves receiving information from the rest of the body, interpreting that information, and then guiding the body’s response to it. Types of input the brain interprets include odors, light, sounds, and pain. The brain also helps perform vital operations such as breathing, maintaining blood pressure, and releasing hormones are just a few of intricacies associated with the brain .The spinal cord functions primarily in the transmission of neural signals between the brain and the rest of the body but also contains neural circuits that can independently control numerous reflexes and central pattern generators.
Another way to think about muscle tone is look at a baby and the moro reflex. This occurs from birth until about 3 months of age. When a baby is held in the supine position and the head is suddenly allowed to fall back, there is symmetrical opening of the arms before they close again (extension then flexion of the limbs). It is a natural defense mechanism to tighten up and prepare for battle or flee.

Interview with my physical therapist located in Marinette, Wisconsin.
I interviewed my physical therapist Kim Barrette who has been like a father figure. He stated, “that my balance was a major problem when Mr. Barrette was performing therapy on me. The success or tremendous phenomenon with you, and a person does not normally see this with patients, is that my balance went from zero to being able to ride a bike. He also goes on to state, “if a person would bet $2 million that Chad Francour in seven years would be able to ride a bike, I would have taken that bet. Dr. Edgar more than likely would not have said seven years post injury you would be able to ride a bicycle. Here, that is a testament at how hard you worked at the rehabilitation. He states, “if you give 100 TBI patients out of that maybe three would be able to ride a bicycle. A special thanks from my physical therapist and me goes to Marinette High School for the letting us perform therapy sessions on the grounds.
Neuromotor impairment is a common symptom of severe traumatic brain injury but has been understudied relative to neurocognitive outcomes. Secondary dystonia is caused by damage from some trauma, medications, infections, or a stroke to the basal ganglia (http://www.neuroanatomy.wisc.edu/coursebook/motor2.pdf). The basal ganglia is associated with a variety of functions, including voluntary motor control, procedural learning relating to routine behaviors or “habits,” eye movements, and cognitive, emotional functions (http://neuroscience.uth.tmc.edu/s3/chapter04.html). Dystonia is represented by sustained contractions of both antagonist and agonist muscles, increase of these involuntary contractions on attempting voluntary movement, rhythmic interruptions, inappropriate or opposing contractions during specific motor actions, and continual movement of a twist in nature.

I however have secondary dystonia. While I Was in a doctors appointment I asked the neurologist, Dr. Terrence Edgar, “how much dystonia do I have?” He stated that I have lost about 80% of muscle control on my left side as compared to 30% on my right side of my body. The reader may wonder what is my gait pattern or the way I walk.
Regarding my motor functioning, I continued to have very significant left upper extremity hemiparesis, with my left arm being essentially nonfunctional. I still ambulate quite slowly. The stance or gait pattern may immediately suggest specific disorders or diseases. In normal locomotion, one leg moves forward and then the other alternately supports the erect moving body. Each leg undergoes periods of acceleration and deceleration is by weight being transferred from one foot to another. When the moving body passes over the supporting leg, the other leg swings forward in preparation for its next support phase. One foot or other consistently contacts the ground and, when support of the body is transferred from the trailing leg to the leading leg, both feet are on the ground momentarily.
Along my left upper extremity paralysis I am forced to wear an arm brace that was made by a specialist. I believe it helps decrease the tightness in my arms because the apparatus keeps my left hand at a neutral position. I also have to walk with a AFO on my left foot whenever I walk long distances, ride a bike, or working out.
Any form of bipedal walking includes two basic requirements: continuous ground reaction forces that support the body’s center of gravity, and periodic movement of the foot from one position of support to the next in the direction of progression.
As a consequence of these basic requirements, certain displacements of the body segments occur regularly in walking. To start walking, a person raises one foot and accelerates the leg forward; this is the swing phase of walking. Muscle action and the supporting leg causes the center of gravity of the body to move forward, creating a horizontal reaction force at the foot. The greater of this reaction force, the greater the acceleration of the body because amount of force is equal to the body mass multiplied by the amount of acceleration. The swing phase ends when the leg that has swung forward is placed on the ground, which is when the stance phase of walking begins. During the stance phase, weight is transferred to the opposite leg in another swing phase can begin. As the body passes over the weight-bearing leg, it tends to be displaced toward the weight-bearing side, causing a slight side to side movement. in addition, the body rises and falls with each step. The body rises to the maximum level during the swing phase and descends to a minimum level during the stance phase. This process is known as the tandem gait pattern.
When a person walks normally, the body should be direct with the head straight and arms are hanging loosely at his or her sides, each moving rhythmically forward with the opposite leg. The shoulders and hips should be approximately level. The arms should swing equally. The central be straight and about equal in length. With each step, the hip and knee should flex smoothly and the angle should dorsiflex with a barely perceptible elevation of the hips as as the toes clear the ground. The heel should strike the ground first and the weight of the body should be transferred successfully onto the sole of the foot and then to the toes.I had in the body should rotate slightly with each step, without lurching or falling. Each person walks in a characteristic fashion. There are gross similarities among people, but a person’s gait reflects physical characteristics and personality traits. Among the variable are speed, stride length, characteristics of walking surface, and the type of footwear worn. Perhaps more important are the person’s inspirations, motivations, and attitudes. The manner of walking may provide clues to personality traits (e.g., aggressiveness, activity, self-confidence, or depression).
Dystonic movements, spasms, and posture can occur from many various causes. When a known pathologic processes present, the disorder is referred to as systematic torsion dystonia. Distonic movements are sustained conditions that are typically twisting in nature and usually increase with action. The spasms can be rapid and repetitive recurring pattern may give the appearance of rhythmicity. With childhood onset, the legs are the most affected site. The dystonic movement of action results in a twisting of leg(s) when a child walks forward,even though walking backward, running, or dancing can still be done normally. As the disorder progresses, the movements appear when the child is at rest; the foot becomes plantar flexed in turn inward. This progression, there is involvement of other limbs and actual muscles the trunk (e.g., scoliosis, lordosis, and tortipelvis) for neck (e.g., torticollis or retrocollis). When the arms are involved, the forearm and rest often show hyperpronation and the arm moves backward (e.g., behind the body) when the patient wants.With adult onset, dystonia usually begins in the arms (e.g., writer’s cramp), neck (e.g., torticollis), or face and jaw (e.g., Meige syndrome). The involvement of open (e.g., spastic dysphonia) is less common.
After extensive research and study dystonia’s pathology is still unknown. Gross examination of the brain and histologic studies have failed to reveal any consistent morphologic changes. In view of this possibility that a biochemical abnormality of the basal ganglia, genetically determines if a person is going to display this disorder. The symptoms may arise from dysfunction within the basal ganglia because CT scans have found evidence of changes in this region. With my dystonia I am a prime candidate for the intrathecal Baclofen pump. Which helps with my gait and somewhat with left upper extremity.
I am now going to shift to my cognitive well-being. Over 95% of right-handed people and most left-handed people are left hemisphere dominant for speech and language. disturbances in speech and language are usually caused by lesions in the region of the brain. Some common problems include errors in cognition (e.g., thinking, memory, and reasoning), sensory processing (e.g., sight, hearing, touch, taste, and smell), communication (e.g., expression and understanding), and behavior or mental health (e.g., depression, anxiety, personality changes, aggression, acting out, and social inappropriateness).
After the hospital I was still left a numerous amount of thinking problems as a result of my trauma. I still displayed a significant moment of dysarthria. Dysarthria is when an individual may have difficulty saying words because of problems with the muscles that help a person talk. A common category for cognitive symptoms after sustaining a traumatic brain injury is aphasia. Aphasia is a neurological disorder caused by damage to the portions of the brain that are responsible for language. This video on aphasia by Cristabelle Braden helps describe this symptom (https://www.youtube.com/watch?v=GkLi-2Obd7w). The amount of disability depends on the location and the severity of the brain damage. Primary signs of the disorder include difficulty in expressing oneself when speaking, trouble understanding speech, and difficulty with reading and or writing. A treatment for aphasia is speech therapy that focuses on relearning and practicing language skills and using alternative or supplementary communication methods.
The first aphasic symptom I will discuss was my paraphasias. Paraphasias is a condition where the patient has problems with the production of speech. The individual may speak fluently, but with grammatical errors. Those errors may range from the mispronunciations of single words to the combination of words in inappropriate or meaningless ways. Because the sounds or words are mixed up, it may be difficult to understand the intended meaning. this symptom is broken up into three categories of paraphasias.
The first is phonemic paraphasias. This symptom is displayed by the substitution, addition, or rearrangement of speech sounds so the error can be identified as sounding like the target. There are three types of paraphasia. An example of this is when a patient says pike but really meant pipe. The second type is known as verbal paraphasias. This type is identified based on whether there is a semantic relationship between the error and the intended word for example, a person sees a wife but says husband. The third is called Neologistic paraphasias. The third type of paraphasias is neologistic. This term is used when a patient speaks words that cannot be identified as having come from the patient’s language. For example, a person sees a toothbrush but he or she says basket (http://www.d.umn.edu/~mmizuko/2230/sym.htm).
The second aphasic symptom that I sometime displayed during my speech and neurology appointments was neologisms. Neologisms is a term used for a word or phrase specifically assigned to a patient. Mine was a hockey player. I love hockey but while in the hospital and shortly after I still thought I would be able to get right back into my hockey career in play again.
Now, here are some neurology documentation from Dr. William Hitch.
The Progression
The date of consultation 06/23/04.
Dear Dr. Turba and Dr. Heida,
Returns today for neurocognitive follow-up. He is currently receiving intensive cognitive retraining at St. Vincent hospital on essentially a daily basis, and my understanding is that this is coming along well. On interview with Chad today, he tells me that he is doing all right; he does note some depression over the breakup of his girlfriend, though Chad implies that he is “handling it.”I see that he is on Zoloft. There were no difficulties in testing in today’s evaluation proceeded without incident.
Test results:
Linguistically,Chad speech has come a long way since his hospitalization, and he is able to verbalize in a significantly more complex way, through overall expression of speech still seems a bit simplistic. His comprehension is full. Overall fluency of his speech is a bit down, but again compared to his hospitalization, speech is showing significant gains. On the measures of verbal intellectual functioning, Chad scored at low average levels at path on mental calculations (WAIS-III) and was actually in the average range of verbal abstraction and analysis. Obviously these scores represent nice improvement from his hospitalization. Turning to his visuospatial domain, Chad scored at borderline levels on a test of visual reasoning, although he was actually able to score in the average range on tasks of higher order perceptual processing (picture arrangement). I was pleased to see this latter score, , since there is a strong executive component to it. Memory remains very problematic: Chad delayed recall lengthy word list (Hopkins) was below the 1st percentile, though it should be noted that Chad is being normed against an age group 6 months his senior. Still, though, I really do not think that this is significant reason for his or score, an obvious memory dysfunction is indicated. On the measures of attention/concentration, Chad scored at borderline levels on the Wechsler Digit Span Test, being able to recycle only three digits and reverse. Concentration obviously remains problematic.
Discussion: Chad is making nice gains in his recovery from his traumatic brain injury, and is significantly improved from his hospital status. His language is improving, though speech is still rather simplistic and not very flowing, and verbal intellectual functioning and visuospatial capabilities have shown nice gains, in fact on certain measures even scorn within normative standards. However, I feel that there is still a lot of room for improvement here. Memory unfortunately remains severely compromised, particularly in terms of delayed recall, though I do feel that the memory is better than it was. In fact, Chad was able to recall some memory test that I gave him during his hospitalization. Still, though, the memory has a long ways to go. Attention/Concentration is currently at borderline levels, particularly for tasks acquiring double tracking and simultaneous manipulation of multiple variables. Behaviorally, Chad was present an interactive, showed a ready smile, and displayed a nice degree of affect.
I would recommend that Chad contained receive intensive kind of retraining through the St. Vincent speech and occupational therapy department. Obviously he remains very significantly impaired, even though nice gains are seen, and is very significantly impaired motor status obviously precludes him from doing certain activities, such as driving, which would be a good idea to stay away from to to the head injury concerns. His family knows that he needs to refrain from any activities that carry any potential risk of head injury. I’ll see Chad again this summer, for more lengthy testing, and will make recommendations at that point regarding possible school issues. For the time being, intensive cognitive retraining is indicated.
Bill hitch, Ph.D., ABPP
Clinical Neuropsychologist
The Progression
Date of Consultation: 08/19/04
Dear Dr. Turba and Dr. Heida,
Chad returns for neurocognitive follow. He continues to receive intensive cognitive retraining from St. Vincent’s Hospital speech therapy and occupational therapy departments, and in addition is received physical therapy. I did speak with Chad’s father, who has noted improvement since I last saw Chad, and we also discussed how high functioning Chad was premorbidly, being on the high honor roll and having a class rank of approximately 20th out of 190 students. Chad was pleasant and cooperative though somewhat impulsive, and today’s testing proceeds without incident.
Test results:
Linguistically, Chad’s speech continue to improve, and he continues to verbalize himself better on more complex subjects. However, there is still a significant amount of dysarthria noted, and though Chad’s speech is improving, and without gross aphasic symptomatology, his overall speech patterns do seem to remain on a simplistic level. Still, though, gains are seen. On measures of verbal intellectual functioning, Chad’s performance today placed him at the average/low average junction (prorated WAIS III V.I.Q. = 90, 25th percentile), with average performances noted on tasks of verbal abstraction and analysis of general fund of knowledge, and low average calculation and digital span scores. The abstraction and calculations or are unchanged from two months ago. Turning to the visuospatial domain, Chad is currently scoring at low average level (prorated WAIS III P.I.Q. = 86), 18th percentile), but it should be noted that this score is disproportionately skewed by a very low performers on a test requiring visuomotor speed and integration (Digital Symbol Coding), which was actually at MR level. If this test is excluded, Chad visuospatial functions are more in the average range, including task assessing visual reasoning, higher-order perceptual processing, and spatial construction. I am seeing improvement in overall visual perception domain, what differences certainly do persist. Chad’s Wechsler Full-Scale IQ score – a generalized index of overall cognitive ability for structured tasks – currently plays in the low average range (prorated WAIS III F.S.I.Q. = 88, 21st percentile). Though the score is certainly a far cry from his premorbid level of functioning, it does represent very nice improvement from earlier and hospitalization and continued gains are anticipated. Chad struggled on tasks of memory. his delayed recollection of paragraph-length information (Wechsler Memory Scale-Revised) was only at the 15th percentile, and his delayed recollection of a lengthy word list (Hopkins) was actually at approximately 5th percentile. Chad’s visual memory also showed impairment: is delayed recollection of geometric stimuli (Wechsler Memory Scale-Revised) was only at the 1st percentile. Through these certainly impaired memory scores, my impression is that Chad has shown improvement in memory functioning from later in his course, as is seen as competitive scores regarding wordless recall.
He continued to have difficulty on tasks of attention/concentration, though improvement is seen. His Digit Span score was below average, as compared to a borderline classification previously, but of note is that he was only able to recite three digits in reverse. He struggled very significantly on the Wechsler Letter Number Sequencing Task, with his score actually placing him at MR levels. It should be noted that Chad was fatiguing rather rapidly when this letter task was administered. Speed of cognitive processing continues to be slow, with Chad actually scoring at MR levels on the Wechsler Digit-Symbol Coding Test. However, his motor and visual difficulty likely contribute to this low score.
Improvement is seen in Chad’s executive capabilities, including complex, novel problem solving and logical, deductive reasoning and analysis. Through his performance on a word generation test (COWAT) was borderline (10 percentile) when he was normed against a young adult age group, he was able to do rather respectably on the Wisconsin Card Sort, considered a cardinal test of executive functioning. He was able to score at average levels on the more complex Wechsler tasks, including visual sequencing in verbal abstraction. I do not have any question that Chad executive capabilities are still very much on the mend, particularly considering the premorbid levels, but I am pleased to see him do as well as he did on today’s testing. Behaviorally, Chad was pleasant and cooperative throughout the evaluation and showed nice comportment. He was rather impulsive, though, it was necessary at many points to ask him to slow down.
Discussion:
Overall neurocognitive status post traumatic brain injury, but still demonstrates significant impairment in multiple areas, particularly when one considers his premorbid stray, high honor roll status. Still, though, his gains to his point are certainly very nice to see, and continued improvement is anticipated.
Briefly reviewing the current neurocognitive profile, Chad speech is I think more fluent but still remains on a somewhat simplistic playing and does show some dysarthria; he is understandable with some effort. Verbal intellectual functioning is currently at the average/low average range, as our overall visuospatial functioning and this does represent some improvement, particularly in the latter area. Chad’s Wechsler Full Scale IQ score That-a journal is index of overall cognitive ability for structured tasks- is at low average levels (prorated WAIS III F.S.I.Q. = 88, 21st percentile) certainly a very significant departure from premorbid capabilities but representative of improvement from earlier in his course. Memory continues to be quite problematic, both for verbal and visual information, especially with delayed recall measures. The visual memory would appear particularly compromise. Though memory is definitely subpar, it does not appear improve from even two months ago. Attention/concentration is also an area of concern, and thankfully Chad is little; hopefully this area will continue to show improvement as he distances itself from the injury. Speed of cognitive processing is slowed, though motor and visual limitations likely exasperate the difficulty. Chad’s executive capabilities and complex, novel problem solving skills have shown very nice improvement from earlier in his course, but I do feel that there is a lot of room for improvement in this dimension. Behaviorally, Chad was pleasant and cooperative, and display full comportment; however, he is rather impulsive.
The plan is for Chad to return to school I have time basis in two weeks. I think that this is appropriate, though it knew few that we have to approach school on a very cautious, tentative trial and error basis to ensure that we do not go too fast and push Chad beyond his capabilities, hence resulting in frustration and possible emotional repercussions. I did discuss this at considerable length with Chad’s father, and he understands completely. I would recommend that Chad attends school in the morning, again only part-time so as to help combat the fatigue that was displayed today during the neurocognitive evaluation. Certainly, if Chad fatigues, his overall performance is going to drop precipitously. This needs to be avoided.I also feel that Chad needs a full-time aide while he is at school, to transition him back into the academic world. Concerning courses, I really think we need to start very cautiously here, enrolling Chad only in rather easy to moderate level classes previously, but I think that this might be premature as things stand now from a cognitive perspective. I would also recommend that Chad receive homebound instruction in the afternoon, preferably after he has had a chance to rest from the morning session. I would also recommend that Chad continue to receive speech and occupational sources through the school. He definitely needs to continue with his Ritalin and to combat his concentration/attention levels.
I would also strongly recommend that Chad’s performance be monitored very closely and that his teachers give feedback to a school contact person, who I can can communicate with to make recommendations accordingly. As stated, it is critical that we do not go to fast here and that Chad be able to handle the scholastic tasks presented to him, and that frustration be avoided. It may be necessary to change sheds curriculum at a very early point, either putting him in less challenging classes or even dropping in class as is needed. Again, very cautious, trial and error approach to ensure that Chad is experiencing success will be important. Both of Chad’s parents are teachers in the same school, and this will help facilitate feedback between teachers and the contact person as well as the parents. I asked Chad’s father to keep in very close contact with me so I can make recommendations accordingly, as well as remaining in contact with school contact individual. I do plan on calling Mr. Dick Hartman, a professional at the school, to discuss Chad’s overall reentry. Clearly, Chad needs to refrain from activities that carry any potential chance of head injury, and I think that this is all low more important with his tendency towards impulsivity and his limited more status. Again, the full-time aide can be quite helpful here. I will continue to follow Chad throughout his reentry into the school, and we will see him for follow-up PRN. I did discuss with the father that this was important to follow Chad’s case longitudinally from a neurocognitive perspective.
Bill hitch, Ph.D., ABPP
Clinical Neuropsychologist
The Progression
Date of the consultation: 12, 29, 2004
Dear Dr. Turba
Chad returned today for neurocognitive follow. He is currently going to school part-time, and brought his report card, which I’m having toward consists of straight A’s In English, History, and chemistry. These are regular curriculum classes, and not special education, which makes Chad’s performance all the more impressive. He is receiving homebound instruction and maintains his dosage of Ritalin. Chad, and his parents, would like to increase his involvement academically, and move to full-time schooling. Testing today proceeded without incident.
Test results:
Linguistically, Chad’s dysarthria has diminished, though it is so readily noticeable. He is able to express himself on more complex levels, and speech is not seen as simplistic as it did previously. I have not seen obvious aphasic symptomatology. On measures of verbal intellectual functioning, Chad is currently scoring just within the average range (WAIS-III V.I.Q. = 91, 27 percentile) which is very close to his performance on these tasks on testing last August.Chad scored within the average range today on task on expressive vocabulary, verbal abstraction and analysis, general fund of knowledge, in social and practical judgment, while mental collations are low average. Again, this performance is similar to the previous testing. On measures of academic achievement (WRAT -R 3), Chad’s scores were considerably in the low average range, including reading, spelling, and arithmetic (reading standard score = 84, 14th percentile; spelling standard score = 85, 16th percentile; arithmetic standard score = 84, 14th percentile). Turning to visuospatial domain, Chad is currently sure once again in the low average range (WAIS-III P.I.Q. = 87, 19th percentile), and once again the score is very comparable to that obtained previously. Chad’s scores were generally cluster on the average range for tasks of visual reasoning, I order perceptual processing, spatial construction, and spatial reasoning, though there was some variability. Visuomotor b and integration remained at MR structure task-currently places him at the upper level and and on the low average range (WAIS-III F.S.I.Q. – 89, 23rd percentile), and once again the score is highly comparable to that obtained four months ago. Chad continues to struggle on tasks of memory functioning. his delay recall of lengthy word list (Hopkins) was at the 2nd percentile, while his you a real collection of a complex visual stimulus (Taylor) was below the 10th percentile. He had difficulty on another visual memory test (DVMT- R), with his delay recollection of geometric stimuli pricing and below the 1st percentile. Attention/concentration looks a little better, and Chad being able to score at the borderline to low average range on the Wechsler Letter Number Sequencing and Digit Span Tasks; on the same task last August his performance was very low. It should be noted that Chad was on Ritalin during today’s evaluation. Speed of cognitive processing remains a major concern with Chad scoring at MR levels on the Wechsler Letter Number Sequencing and Digit Span, with little improvement seen in either of these areas.
Finally, Chad performances on tasks of executive functioning-complex, novel problem solving, and cognitive ability and flexibility-were inconsistent. He did handle the Wisconsin Card Sort considered a cardinal test of executive functions-at normal levels, and also able to score on average range of more complicated Wechsler tasks, including verbal abstraction And visual sequencing. In contrast, though, Chad performance on the Short Category Test was very poor (1st percentile), and on word generalization test (COWAT), his performance was only at the 5th percentile, a deficient ranking. Behavior really, he was pleasant and cooperative and showed full cooperation throughout the evaluation.
Discussion:
Today’s tests are fairly consistent with those obtained in testing four months ago, and continue indicated Chad has difficulty on tasks of complex memory, speed of cognitive processing, and executive functioning. In addition, attention/concentration, verbal reasoning, and visuospatial functions still all appeared to be subpar relative to premorbid capabilities, particularly since Chad was a high honor roll student. Chad continues to have left hemiplegia, and is quite limited motorically, particularly in terms of speed.
Briefly reviewing the current neurocognitive profile, Chad’s language still demonstrates a dysarthria, though overall I feel that he is able to express himself at a higher level. Verbal intellectual functioning is just within the average range, while visuospatial capabilities are low average, With both areas showing close similarities to performances obtained in the last evaluation. Chad’s memory for verbal and visual information remains compromised, particularly for tasks that are lengthy or complex. Again, today’s test scores do seem similar to those obtained for months ago. Attention/concentration I do think this is a little better but speed of cognition remains very very slow. Clinically, Chad’s parents nor that the processing speed issue remains rather paramount. Chad performed inconsistently in tests of executive functioning, a time is performing within normal limits, while at other times struggling. Behaviorally, he was pleasant and cooperative and show full cooperation.
In spite of the similarity between today’s test results in the looking glass August, and despite the fact that Chad still demonstrates very significant neurocognitive compromise in multiple areas, I think that his very fine performance academically is a good measure of how he can do with assistance in extra help, and Chad certainly needs to be applauded for his fine performance. I did renounce this to him repeatedly. Chad very much wants to move up to a full time level of schooling in based on how well he has done in the past four months in the school system, I think this is appropriate. Consequently, I am in favor of him adding economics and trigonometry, though I stress to Chad and his parents that, this is a heavy course load, and that these are exactly were the subjects; however, again Chad has done very well with teacher courses based on his performance to this point and with school support. Certainly, we do not want to frustrate Chad with assistance hopefully he will be listed do well. Chad also would like to fix a CT test, and certainly he should be given extra time to take this examination, particularly with his feet of processing difficulties. I would be happy to write a letter in Chad’s behalf regarding the necessity of this as such is required. I would also recommend continuation of Ritalin, sense I think it is likely helping them significantly. In addition to full-time schooling I would strongly recommend that Chad continued to receive homebound instruction, and that he continues to receive in school aid through the use of a paraprofessional. I discussed this at length with his parents, and stress that I did not think he should change anything in terms of academic assistance cents Chad is doing so well. Certainly I would recommend that you continue to receive I fish of therapy, speech therapy, and physical therapy.
Regarding his emotional situation, Chad flatly denies any depression, and indeed tells me that he is doing good in terms of overall emotional situation. He promised that he would contact me or a primary care physician if compression ever became an issue. Chad’s parents tell me that, thankfully, he has maintained his relationships, and that friends continue to include in the in activities.
As always I would be happy to discuss Chad’s situation with school professionals and I think that they are to be lauded for excellent job they have done in helping Chad reenter into the school environment and prosper economically, and spite of his neurocognitive difficulties.
Bill hitch, Ph.D., ABPP
Clinical Neuropsychologist
The Progression
Date of Consultation: 08/03/05
Dear Dr. Turbra
Chad returns today for neurocognitive follow-up. Chad did take a five credit load this past semester, and unfortunately this did appear to be too much, with Chad showing a mild drop in grades but, of more importance, showing concerns with overall emotional functioning, problems with peer relationships, inquiring excessive effort to get the grades he received. The mother noted that he tended to become somewhat depressed, and even at the one point voice some suicidal ideation. Currently, States that he feels “good” emotionally, and flatly denies any depression. He is currently on Concerta, and evidently this is helping him. I have been in contact with the school district of Marinette office of student services, suggesting that he continues to receive tutorial assistance and a paraprofessional to help them with his class work. There were no difficulties in testing Chad in today’s test proceed without incident.
Test results:
Linguistically, I think that Chad dysarthria is improved, though it is still quite evident, observationally. Otherwise, though, I really do not see aphasia concerns. He does speak rather slowly at times. On measures of verbal intellectual functioning, Chad is currently scoring once again just within the average range (prorated WAIS-III VIQ = 91, 27th percentile), and this score is identical to that obtained in testing a month ago, primarily with respect to verbal abstractions, mental calculations, and digit span. Chad’s visuospatial capabilities are currently within the average range (prorated WAIS-III PIQ = 100, 50th percentile), but only if speed tasks are deleted, which otherwise disproportionately skew overall PIQ score. Chad was able to score at normal levels today on task of perceptual reasoning and spatial structuring, and was at average to upper average levels in the last testing on higher-order perceptual processing and visual reasoning. However, visuomotor speed and integration as measured by digit symbol coding was at MR levels. Overall, I do feel that he has shown improvement in the visuospatial domain, particularly cents, in the last testing, he was at low average levels (PIQ = 87, 19th percentile), though again speed considerations need to be made. Chad Wechsler full-scale IQ score – a generalized index of overall cognitive ability for constructive tasks – currently places him within average limits (prorated WAIS- III FSIQ = 95, 37th percentile); this score is a bit higher than that obtained in the last evaluation (FSIQ = 89, 23rd percentile).
Chad continues to have difficulty on complex test of verbal memory. His delayed of a lengthy word list (Hopkins) was at the 2nd percentile, though he did benefit very well from prompting in queuing. His score on this task is identical to that obtained last December on a similar measure. Visual memory, however, look significantly improved: Chad’s delayed recall of a complex usual stimulus (Rey-Osterreith) was within normal limits (32nd percentile), on a similar test match evaluation his performance was below the 10th percentile. Attention/concentration remains problematic: chads scored at the low average/borderline range of task a letter-number sequencing and digit span, not significantly improve from last testing. It should be noted that he was on a concert during the evaluation. Speed of cognitive processing, as stated, remains a major concern, and indeed Chad scored at borderline to MR levels on the Wechsler symbol search and digit symbol coding tests. Chad slow speed of cognitive processing is obviously. Finally, Chad has shown improvement in executive functioning/complex problem-solving: his performance on the short category test today was at the 54th percentile as compared to the 1st percentile ranking on this measure last December. However, Chad performance on a word generation test (FAS) remained far below the normal (10th percentile, borderline) though it was improved from eight months ago(defiant ranking, 5th percentile). Behaviorally, he was pleasant and cooperative and displayed full comportment.
Discussion:
I think that Chad has made improvements in his overall neurocognitive functioning sense I saw him last December, though he continues to demonstrate very significant concerns with speed of cognitive processing, attention/concentration, and verbal memory. His performances in verbal intellectual functioning and visuospatial capabilities, as well as executive functioning, are generally close to or at the average range, though executive impairments are noteworthy on specific tasks; though such a ranking certainly represents significant gains for Chad immediately post trauma, they are obviously significantly below his previous level of functioning, since he was a straight A, high honor roll student.
I would recommend that Chad continue with Concerta, and even that consideration for upping the dose he made if this is feasible, based on his continued difficulties with processing speed and attention. He is set to enter his senior year in the fall, taking rather challenging courses (anatomy/physiology, advanced algebra, and English), but he will continue receiving tutorial assistance as well as help from a paraprofessional, which I think is absolutely indicated. Obviously, if cat encounters significant difficulty, arrangements in in his academic program will need to be made. I would ask that his parents keep me posted on his progress, and of course I would be happy to speak with school personnel regarding this situation. The plan is he is considering college, possibly the University of Minnesota maybe after spending two years at the UW Marinette extension. College would certainly be a challenge, based on today’s test scores, but my feeling is we should let Chad’s performance speaks for itself, and make plans and arrangements accordingly, tailoring these plans to meet Chad’s ability to handle the academic situation. His performance over the coming years should give a good indication of whether or not he is able to handle college, again with respect to his performance level. I will see Chad for follow-up this winter and get information right over to you. Certainly, it will be important to monitor Chad’s overall level of emotional functioning, though he states he is doing well at this point. I would ask the parents to keep me posted regarding the emotional situation as well.
Bill hitch, Ph.D., ABPP
Clinical Neuropsychologist
Lastly, is my social aspect of my injury. To understand my social paralysis would be very difficult if I did not explain my life before the accident. As a reader can presume I was well-liked among my peers and in the community. I was actively involved in athletics and other social gatherings. So what is the end result of suffering a traumatic brain injury in high school? I address my friendships, social communication both verbal and nonverbal, problems, who cares, and confidence.
Being well liked, I believe, that other individuals either felt sympathy or obligated to remain in contact with me. Using a existential perspective on my friends would be very intelligent. If the reader does not know about existential theory I will try my best to explain it. Essential theory states that one’s thoughts or actions are both conscious and non-conscious in his or her mind. I bring this up because I feel the losing of my friends may have been intentional or unintentional or my thinking could just be a defense mechanism for myself. I will explain my rationale.
I stated that the losing of my friends could have been deliberate or indirect because of the traumatic brain injury. I, however, like to think that the losing of my friends was because he or she was looking out for the best interest of myself. If, for example, my friends wanted to go out and drink alcohol, he or she thought that drinking alcohol could possibly damage my brain. My friends did not want that to happen so he or she did not invite me out to a party. Then a reader can apply the existentialism theory as an almost defense mechanism for my own self worth.
Another aspect to consider is my life changed dramatically. I was constantly having therapy, doctors appointments, overprotective parents, or paraprofessionals in school and that was is not, “normal” in a high schoolers life. I just could not partake in the similar hobbies as my friends. When a person is 16 years of age he or she lives life by the seat of their own pants. Meaning, that a lot of plans are set up at the last minute which results in a fast-paced lifestyle. I do not have the ability to just pack up and go at my free will. I do not hold any resentment or dislike towards my high school friends because that is just life. Every person will eventually mature into an adult sooner or later.
There may also be a negative aspect to my situation. I could have been just not well liked because I could have been a bully. Now, I would not be out right mean but I stuck around my social group and stayed that way for my teenage years. My peers would have been jealous of me before the accident and now are implicitly jealous after the accident.
I had numerous amount of acquaintances after my accident. I say acquaintances because those people would not include me on such activities (e.g., hunting, partying, or going to sporting events) because he or she thought that I could not do the activity. Pretty much I had my two parents and my dogs to count on. It is funny because when I think about my dogs I say, “I love them unendlessly.” Mali and Bella have always been there for me to pet or play catch with outside. A side note, has the reader ever heard the saying, “after a while a dog personality and appearance becomes similar to that of the owner.” Mali’s, named after a country in Africa close to Chad and Kenya, personality is faithful, hard-working, and willing to have fun. I say faithful because she is always around me. She knows when my car pulls up to the driveway and is always excited to see me with a wagging tail. She does not care that I have a disability or am cognitively slower; all my labradooble cares about is me and only me. I say only me because she is not friendly to other individuals. Mali is very smart; she went through a dog training Academy in my local town. Her mother was the first labradooble who was a seeing-eye dog.

Is she not adorable?
It is important to be cognizant of the age at which my accident occurred. I was 16, a prime time where my peers were engaging in interesting (e.g., cars, friends, and romantic partners) ventures. I do not hold any hostility towards my friends because I am a better person because I did not get bogged down with all the high school drama. What other problems does a traumatic brain injury individual commonly suffer from?
Depending on the location and severity of a person’s injury to the brain may indicate some of the social issues that may accompany a patient. Because of the complexity of the brain I am only going to focus on the basic structures and functions of each.

Starting off with the frontal lobe, the structure is one of the four major divisions of the cerebral cortex. This part of the brain regulates decision making, problem solving, control of purposeful behaviors, consciousness, and emotions. The primary motor cortex is part of the frontal lobe and is responsible for regulating voluntary movements. If an individual experiences a brain injury in this structure he or she might experience poor decision-making, difficulties with problem solving, inability to control behaviors and/or emotions. Another possibility is ability to make voluntary movement. If this part is damaged, likewise, an individual might not be able to move freely. This part of the brain is responsible for rational thought and is where all the higher cognitive thinking takes place.
The temporal lobe is a part of the brain that regulates memory, emotions, hearing, language, and learning. If a patient has damage in the temporal lobes there are eight distinct symptoms. The first is
Kolb and Wishaw (1990) have identified eight principle symptoms of temporal lobe damage: 1) disturbance of auditory sensation and perception, 2) disturbance of selective attention of auditory and visual input, 3) disorders of visual perception, 4) impaired organization and categorization of verbal material, 5) disturbance of language comprehension, 6) impaired long-term memory, 7) altered personality and affective behavior, 8) altered sexual behavior.
Selective attention to visual or auditory input is common with damage to the temporal lobes (Milner, 1968). Left side lesions result in decreased recall of verbal and visual content, including speech perception. Right side lesions result in decreased recognition of tonal sequences and many musical abilities. Right side lesions can also affect recognition of visual content (e.g. recall of faces). The temporal lobes are involved in the primary organization of sensory input (Read, 1981). Individuals with temporal lobes lesions have difficulty placing words or pictures into categories. Language can be affected by temporal lobe damage. Left temporal lesions disturb recognition of words. Right temporal damage can cause a loss of inhibition of talking.
The temporal lobes are highly associated with memory skills. Left temporal lesions result in impaired memory for verbal material. Right side lesions result in recall of non-verbal material, such as music and drawings. Seizures of the temporal lobe can have dramatic effects on an individual’s personality. Temporal lobe epilepsy can cause perseverative speech, paranoia and aggressive rages (Blumer and Benson, 1975). Severe damage to the temporal lobes can also alter sexual behavior (e.g. increase in activity) (Blumer and Walker, 1975).
The parietal lobe is at the back of the brain and is divided into two hemispheres. It functions in processing sensory information regarding the location of parts of the body as well as interpreting visual information and processing language and mathematics.
References:
Blumer, D., & Benson, D. Personality changes with frontal and temporal lesions. In D.F. Benson and F. Blumer, eds. Psychiatric Aspects of Neurologic Disease. New York: Grune & Stratton, 1975.
Blumer, D., & Walker, E. The neural basis of sexual behavior. In D.F. Benson and F. Blumer, eds. Psychiatric Aspects of Neurologic Disease. New York: Grune & Stratton, 1975.
Kolb, B., & Whishaw, I. (1990). Fundamentals of Human Neuropsychology. W.H. Freeman and Co., New York.
Milner, B. (1968). Visual recognition and recall after right temporal lobe excision in man. Neuropsychologia, 6:191-209.
Milner, B. (1975). Psychological aspects of focal epilepsy and its neurosurgical management. Advances in Neurology, 8:299-321.
Read, D. (1981). Solving deductive-reasoning problems after unilateral temporal lobectomy. Brain and Language, 12:116-127.
Taylor, L. (1969). Localization of cerebral lesions by psychological testing. Clinical Neurosurgery, 16:269-287.
MORE WILL COME……
Leave a Reply